Medical Cannabis for Peripheral Neuropathy Treatment – Part 3 of 5
This is the third of five articles on medical cannabis and its use as a peripheral neuropathy treatment.
How Does Cannabis Work
by Dr. Rosemary Mazanet
In Part 2 of this series we described the history of cannabis and explained that there are two different species: Cannabis Indica and Cannabis Sativa. This installment will describe how each of these strains are used as a peripheral neuropathy treatment.
Scientists have determined that genetic differences between the two strains result in the production of a predominant amount of a particular chemical (called a cannabinoid) such as THC or CBD. The amounts of THC or CBD, as well as the numerous secondary components present in smaller amounts that may also provide unique benefits determine how the cannabis plants are recommended for different medicinal purposes. Today’s pharmaceutical-grade medical cannabis (nonflower) is usually designated by its THC:CBD ratio.
Main uses for THC:CBD Ratios
THD Predominant
- Analgesic/”Opiate Type Pain Relief”
- Appetite Stimulant
- Nausea
- Sleep
- Muscle Relaxation
CBD Predominant
- Neuropathic Pain Relief
- Anti-Inflammatory
- Anxiolytic
- Cytotoxic
- Antispasmodic
- Anticonvulsant/Seizures
Cannabis Effects on Human Physiology
It wasn’t until the mid-1990s that scientists discovered WHY marijuana exerts so many effects in the human body. The body makes its own endocannabinoids (i.e., anandamide, 2-AG), which are part of a system, the Endocannabinoid System that influences multiple physiological processes such as:
- Modulation of Pain
- Seizure threshold
- Appetite
- Inflammation
- Mood
- Regulation of Immune system
- Tumor surveillance
- Intraocular pressure
- Bone physiology
- Digestion
These endocannabinoids circulate in the blood stream and bind to cannabinoid receptors in order to have their effect. The amounts of endocannabinoids that are physiologic in humans is low enough to not have euphoric or central nervous system effects that are apparent.
There are currently two subtypes of cannabinoid receptors that are well characterized. The CB1 receptors are highly concentrated in the brain and nerve endings and the CB2 receptor is expressed mainly on cells of the immune system and blood forming cells. There are also less well understood VR1 receptors.
Understanding the Endocannabinoid System
Cannabinoid Receptor-1 (CB1)
- Highly expressed in the brain and CNS
- Responsible for Neurotransmitter Release
- Glutamate, GABA, Serotonin, Dopamine, Acetylcholine, Neuropeptides
- Pain, motor control, memory processing, appetite, spasticity, circulatory effects, emesis, epilepsy, anxiety, etc.
- Not prevalent in the brainstem, which may account for lack of cannabis-related fatalities (i.e. respiratory depression)
- 10 times more prevalent in the CNS as compared to μ-opioid receptor for narcotics
Cannabinoid Receptor-2 (CB2)
- Highly expressed in immune cells
- Modulation of Cytokine Release
- Immune Responses and Anti-inflammatory effects
Vanilloid Receptor (VR1) (also known as Transient Receptor Potential Vanilloid Receptor or TRPV1)
- Highly expressed in the CNS
- Responsible for Nociception
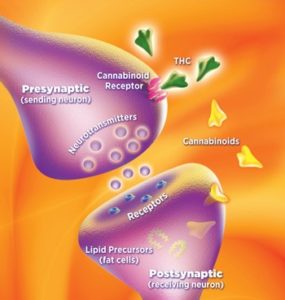
The cannabinoids in agricultural cannabis or marijuana (Phytocannabinoids, i.e. THC, CBD) bind and activate or inactivate these receptors in the body in much the same way as the human produced endocannabinoids do, at the receptor. When THC enters the blood stream and reaches the brain, it binds to CB1 receptors much the same way as an endocannabinoid would (like in Figure 4), except at a pharmacological dose rather than a physiological dose. This type of binding results in changes in the levels of various neurotransmitters (like dopamine and norepinephrine) released from the neurons. The result for the patient is the acute effects of cannabis ingestion, such as euphoria and anxiety.
There are two subtypes of cannabinoid receptors that are currently well characterized. The CB1 receptors are highly concentrated in the brain and nerve endings and the CB2 receptor is expressed mainly on cells of the immune system and blood forming cells. There are also less well understood VR1 receptors.
Unlike the psychoactive THC, CBD has little binding affinity to either the CB1 or CB2 receptors. Instead, CBD reduces the breakdown of the endocannabinoids the body has already made, indirectly increasing their amount and normal activity at the receptors. At the same time, CBD opposes the action of THC at the CB1 receptor, thereby muting the psychoactive effects of THC.
Potential Therapeutic Properties of Medical Cannabis for Neuropathic Pain
THC
- has “Opiate-type Pain relief”/Opiate Sparing
- Anti-inflammatory
CBD
- Neuropathic Pain relief
- Anti-inflammatory
- Patient Specific
- CBD provides neuropathic pain relief, most patients should benefit
Ratios Most Beneficial for Neuropathic Pain is Patient Specific
- Minimal THC may be better for THC naïve patients, or patients wanting to avoid THC related side effects
- Increased THC may be beneficial for patients using opiates for pain, or experiencing insomnia related to pain
Low THC : V. High CBD
- Treatment of Neuropathic pain for patients wanting to avoid THC-related side effects
- Epilepsy in children
Low THC : High CBD
- Treatment of Neuropathic pain in THC naïve patients
- For patients wanting to minimize THC-related side effects
1:1 Equal THC/CBD
- Treatment of Neuropathic pain in patients who use opiates to treat pain
High THC : Low CBD
- Severe pain relief & sleep
- For patients who use opiates to treat pain
- Patients may experience insomnia from the use of CBD’s
This is the third in a series of five articles on medical cannabis by Dr. Mazanet for the Foundation for Peripheral Neuropathy:
- The Status of Legalized Medical Marijuana and What is Dispensed
- The History of Cannabis Use
- How Does Cannabis Work?
- The Benefits and Effects of Medical Cannabis
- How to Use Medical Cannabis
About the author: Dr. Rosemary Mazanet, MD, PhD, was trained in Internal Medicine (Brigham and Women’s Hospital, Boston) and Medical Oncology (Dana Farber Cancer Institute, Boston), and has been active in the Biotechnology community for the last 30 years. Currently she is involved in strategic drug development and is the head of the Scientific Advisory Board for Columbia Care, Inc, a company that grows and dispenses legal medical cannabis in nine states.